Ever wondered how a simple ECG can reveal the secrets of your heart? Let’s dive into the world of leads on ECG and uncover what they really mean for heart health.
Understanding Leads on ECG: The Basics

When it comes to diagnosing heart conditions, the electrocardiogram (ECG or EKG) is one of the most fundamental tools in modern medicine. At the heart of this diagnostic method—pun intended—are the leads on ecg. These leads are not physical wires leading to the heart, but rather specific electrical viewpoints that capture the heart’s activity from different angles. Each lead provides a unique perspective, allowing doctors to analyze the direction and magnitude of electrical impulses as they travel through the cardiac muscle.
The standard 12-lead ECG is the most commonly used format in clinical settings. It combines information from 12 different leads—each representing a distinct vector of electrical activity. These leads are derived from just 10 electrodes placed on the patient’s limbs and chest. Understanding how these leads work is essential for interpreting ECG results accurately and diagnosing conditions like arrhythmias, myocardial infarctions, and conduction abnormalities.
What Are Leads on ECG?
In ECG terminology, a “lead” refers to a specific combination of electrodes that measures the voltage difference between two or more points on the body. This voltage difference reflects the electrical activity of the heart as it depolarizes and repolarizes during each heartbeat. The term can be confusing because, although there are only 10 physical electrodes, the machine calculates 12 different leads by combining signals in various ways.
For example, Lead I measures the voltage between the right and left arms, while Lead II compares the right arm to the left leg. These leads are part of the limb lead system, which includes both bipolar (measuring between two electrodes) and augmented unipolar leads. The chest (precordial) leads, labeled V1 through V6, are placed across the chest wall and provide a horizontal view of the heart’s electrical activity.
“The 12-lead ECG is the cornerstone of cardiac diagnosis—it’s fast, non-invasive, and incredibly informative when interpreted correctly.” — American Heart Association
Types of Leads: Limb vs. Precordial
The 12 leads on ECG are divided into two main groups: the limb leads and the precordial (chest) leads. The limb leads consist of six leads—three standard bipolar leads (I, II, III) and three augmented unipolar leads (aVR, aVL, aVF). These leads primarily provide a vertical or frontal plane view of the heart’s electrical activity.
- Standard Limb Leads: Lead I (right arm to left arm), Lead II (right arm to left leg), Lead III (left arm to left leg).
- Augmented Limb Leads: aVR (augmented vector right), aVL (augmented vector left), aVF (augmented vector foot). These are unipolar leads that use a single positive electrode and a reference point derived from the other two limbs.
The precordial leads (V1–V6) are placed across the chest in specific anatomical positions. They offer a horizontal plane view of the heart, focusing on the anterior, lateral, and septal walls. Because they are positioned close to the heart, they are especially sensitive to changes in the ventricles.
How Leads on ECG Capture Heart Activity
Each lead on an ECG records the electrical activity of the heart from a specific angle. When the heart depolarizes, the wave of electrical activity moves through the atria and then the ventricles. Depending on the direction of this wave relative to a given lead, the deflection on the ECG tracing will be positive, negative, or isoelectric (flat).
For instance, if the electrical impulse travels toward the positive electrode of a lead, it produces an upward (positive) deflection. If it moves away, the deflection is downward (negative). This principle allows clinicians to determine the heart’s electrical axis—the overall direction of depolarization in the frontal plane—by analyzing the net deflection in leads I and aVF.
Understanding how leads on ecg capture this data is crucial for identifying abnormalities. For example, a deep Q wave in leads II, III, and aVF may indicate an inferior wall myocardial infarction, while ST-segment elevation in V1–V3 could suggest an anterior infarction.
The 12-Lead ECG System Explained
The 12-lead ECG system is the gold standard for non-invasive cardiac assessment. It provides a comprehensive view of the heart’s electrical activity by combining information from multiple leads. Each lead contributes unique data that, when analyzed together, allows for precise localization of cardiac abnormalities.
This system is based on the Einthoven triangle, a conceptual model developed by Willem Einthoven in the early 20th century. The triangle is formed by the placement of electrodes on the right arm, left arm, and left leg. Leads I, II, and III are derived from this triangle and form the foundation of the limb lead system.
Einthoven’s Triangle and the Law of Einthoven
Einthoven’s Triangle is a foundational concept in understanding leads on ecg. It represents the three standard limb leads (I, II, III) as the sides of an equilateral triangle, with the heart at the center. Each lead measures the potential difference between two limbs:
- Lead I: Left arm – Right arm
- Lead II: Left leg – Right arm
- Lead III: Left leg – Left arm
The Law of Einthoven states that the voltage in Lead II is equal to the sum of the voltages in Lead I and Lead III (i.e., II = I + III). This mathematical relationship helps verify the accuracy of ECG recordings and is used in troubleshooting lead placement errors.
For more on Einthoven’s contributions, visit the Nobel Prize biography of Willem Einthoven.
Augmented Limb Leads: aVR, aVL, aVF
While the standard limb leads are bipolar, the augmented leads (aVR, aVL, aVF) are unipolar, meaning they use a single positive electrode and a combined reference point from the other two limbs. These leads provide additional perspectives on the heart’s frontal plane activity.
- aVR: Looks at the heart from the right shoulder. It’s often inverted in normal ECGs because the main electrical forces move away from this lead.
- aVL: Views the lateral wall of the left ventricle.
- aVF: Focuses on the inferior wall of the heart.
These leads are particularly useful in determining the electrical axis and identifying inferior or lateral myocardial infarctions. For example, ST elevation in aVF and Lead II may indicate an inferior MI.
Precordial (Chest) Leads V1 to V6
The precordial leads are placed across the chest in a specific sequence:
- V1: 4th intercostal space, right sternal border
- V2: 4th intercostal space, left sternal border
- V3: Midway between V2 and V4
- V4: 5th intercostal space, midclavicular line
- V5: Anterior axillary line, same horizontal level as V4
- V6: Midaxillary line, same level as V4
These leads provide a horizontal view of the heart. V1 and V2 are close to the right ventricle and interventricular septum, making them ideal for detecting right-sided issues or septal infarcts. V5 and V6, being over the left ventricle, are key in diagnosing lateral wall ischemia.
Abnormalities in the precordial leads—such as deep S waves in V1 or tall R waves in V5—can indicate ventricular hypertrophy or bundle branch blocks.
How Leads on ECG Help Diagnose Heart Conditions
The power of leads on ecg lies in their ability to localize cardiac pathology. By analyzing which leads show abnormalities, clinicians can pinpoint the affected area of the heart. This spatial resolution is what makes the 12-lead ECG so valuable in emergency and outpatient settings.
For example, during an acute myocardial infarction, the location of ST-segment elevation or depression across different leads can indicate which coronary artery is blocked. This information guides immediate interventions like thrombolytic therapy or percutaneous coronary intervention (PCI).
Identifying Myocardial Infarction Using Leads
One of the most critical applications of leads on ecg is in diagnosing myocardial infarction (MI). The leads involved determine the location of the infarct:
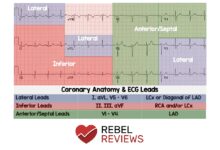
- Inferior MI: ST elevation in II, III, aVF
- Anterior MI: ST elevation in V1–V4
- Lateral MI: ST elevation in I, aVL, V5–V6
- Septal MI: ST elevation in V1–V2
- Posterior MI: Often seen as tall R waves and ST depression in V1–V3 (confirmed with posterior leads V7–V9)
Reciprocal changes—such as ST depression in leads opposite the infarct zone—also support the diagnosis. For instance, ST depression in aVL may accompany an inferior MI.
Learn more about MI diagnosis at American Heart Association – Heart Attack.
Detecting Arrhythmias Through Lead Patterns
Arrhythmias, or irregular heart rhythms, can also be identified through leads on ecg. Different leads help distinguish between supraventricular and ventricular arrhythmias.
- Atrial fibrillation: Irregularly irregular rhythm, absent P waves, best seen in Lead II and V1.
- Ventricular tachycardia: Wide QRS complexes, often with AV dissociation, visible in multiple leads but especially clear in V1.
- Bradycardia: Slow heart rate, may show in all leads, but P wave morphology in II and aVR helps determine origin.
Lead V1 is particularly useful for identifying P wave abnormalities and differentiating between types of tachycardia.
Recognizing Hypertrophy and Enlargement
Left ventricular hypertrophy (LVH) and right ventricular hypertrophy (RVH) can be detected using specific criteria across multiple leads on ecg.
- LVH: Sokolow-Lyon criteria: S in V1 + R in V5 or V6 > 35 mm. Also, Cornell voltage criteria: R in aVL + S in V3 > 28 mm (men) or > 20 mm (women).
- RVH: Tall R wave in V1 (>7 mm), R/S ratio >1 in V1, deep S in V5–V6, right axis deviation.
Atrial enlargement can also be detected: P mitrale (broad, notched P waves in II) suggests left atrial enlargement, while P pulmonale (tall, peaked P waves in II) indicates right atrial enlargement.
Proper Electrode Placement for Accurate Leads on ECG
Even the most advanced ECG machine cannot compensate for incorrect electrode placement. Misplaced electrodes can lead to misinterpretation, false diagnoses, and inappropriate treatment. Therefore, precise placement is critical for accurate leads on ecg readings.
The standard 10-electrode setup must follow strict anatomical landmarks. Deviations of even a few centimeters can alter the appearance of the ECG, especially in the precordial leads.
Limb Lead Placement Guidelines
Limb electrodes should be placed on the distal parts of the limbs—on the wrists and ankles—but not directly on the joints. For ambulatory patients, they are often placed on the upper arms and lower legs to avoid movement artifacts.
- Right Arm (RA): On the right wrist or upper arm.
- Left Arm (LA): On the left wrist or upper arm.
- Right Leg (RL): On the right ankle or lower leg (ground electrode).
- Left Leg (LL): On the left ankle or lower leg.
It’s essential to ensure good skin contact by cleaning the area and using conductive gel if necessary. Poor contact can cause baseline wander or noise.
Chest Lead Placement: V1 to V6
The precordial leads require precise anatomical placement:
- V1: 4th intercostal space, right sternal border.
- V2: 4th intercostal space, left sternal border.
- V3: Midway between V2 and V4.
- V4: 5th intercostal space, midclavicular line.
- V5: Same horizontal level as V4, anterior axillary line.
- V6: Same level as V4, midaxillary line.
Misplacement of V1 and V2 too high or too lateral can mimic anterior MI or mask true abnormalities. Similarly, incorrect V4 placement can affect the diagnosis of LVH.
“A misplaced electrode can mimic a heart attack. Precision saves lives.” — Dr. Eric Topol, Scripps Research
Common Placement Errors and How to Avoid Them
Some of the most frequent errors include:
- Swapping left and right arm electrodes: This inverts Lead I and can mimic dextrocardia.
- Placing V4 too low: Can cause false ST elevation.
- Incorrect intercostal space identification: Especially in obese or elderly patients.
- Reversing V5 and V6: May alter QRS progression.
To avoid these, always palpate bony landmarks, use anatomical references (like the angle of Louis for the 2nd rib), and double-check placements before recording.
Advanced Interpretation of Leads on ECG
While basic ECG interpretation focuses on rhythm and obvious infarcts, advanced analysis of leads on ecg involves assessing subtle changes, axis deviation, and waveform morphology. This level of detail is essential for nuanced diagnoses.
For example, a slight ST depression in multiple leads might indicate subendocardial ischemia, while a subtle Q wave in aVL could be the only sign of a prior lateral MI.
Electrical Axis Determination Using Leads
The heart’s electrical axis represents the overall direction of ventricular depolarization in the frontal plane. It’s determined using the limb leads, particularly I and aVF.
- Normal axis: -30° to +90°
- Left axis deviation: -30° to -90° (seen in left anterior fascicular block, LVH)
- Right axis deviation: +90° to +180° (seen in RVH, chronic lung disease)
- Extreme axis: -90° to +180° (rare, may indicate ventricular rhythm)
To estimate the axis, find the lead with the most isoelectric QRS (equal positive and negative deflection). The axis is perpendicular to that lead. For instance, if Lead I is isoelectric, the axis is ±90° (either +90° or -90°), and you check aVF to determine direction.
Waveform Analysis Across Multiple Leads
Each component of the ECG waveform—P wave, QRS complex, ST segment, T wave—should be analyzed in all 12 leads for consistency and abnormalities.
- P wave: Should be upright in I, II, aVF; inverted in aVR. Abnormalities suggest atrial issues.
- QRS complex: Duration should be <120 ms. Widening suggests bundle branch blocks or ventricular rhythms.
- ST segment: Should be isoelectric. Elevation or depression indicates ischemia or infarction.
- T wave: Should be upright in most leads. Inversion may indicate ischemia, hypertrophy, or electrolyte imbalances.
For example, T wave inversion in V1–V3 is normal in young individuals but may indicate ischemia in older patients.
Recognizing Lead Reversal Artifacts
Lead reversals are common artifacts that can mimic pathology. The most frequent is right-left arm reversal, which causes:
- Inverted P waves, QRS, and T waves in Lead I
- Positive QRS in aVR
- Resemblance to dextrocardia
Clues to reversal include aVL and aVR appearing swapped and Lead II and III being switched. Always check for consistent P wave morphology across leads to detect such errors.
Clinical Applications of Leads on ECG in Emergency Medicine
In emergency departments, leads on ecg are often the first diagnostic tool used for patients with chest pain, palpitations, or syncope. Rapid interpretation can mean the difference between life and death.
Protocols like the “12-lead ECG within 10 minutes of arrival” for suspected MI are standard in chest pain centers.
ECG in Acute Coronary Syndrome
Acute coronary syndrome (ACS) includes unstable angina, NSTEMI, and STEMI. The 12-lead ECG is critical in differentiating these:
- STEMI: ST elevation ≥1 mm in two contiguous leads (≥2 mm in V1–V3 in men, ≥1.5 mm in women).
- NSTEMI: No ST elevation, but may have ST depression or T wave inversion.
- Unstable angina: Non-diagnostic changes, but high clinical suspicion.
Immediate reperfusion therapy is indicated for STEMI, making rapid ECG interpretation vital.
For current ACS guidelines, refer to the ACC/AHA Guidelines.
Use of Leads on ECG in Arrhythmia Management
In arrhythmia cases, leads on ecg help determine the origin and mechanism of the rhythm. For example:
- Narrow QRS tachycardia: Likely supraventricular (SVT).
- Wide QRS tachycardia: Could be VT or SVT with aberrancy—V1 morphology helps differentiate.
Brugada pattern in V1–V3 (coved ST elevation) may indicate a risk for sudden cardiac death.
Monitoring Cardiac Changes Over Time
Serial ECGs using consistent leads on ecg placement allow clinicians to monitor disease progression or response to treatment. For example:
- Resolving ST elevation after thrombolysis confirms reperfusion.
- New left bundle branch block may prompt urgent angiography.
- Progressive QT prolongation may indicate drug toxicity.
Consistency in lead placement and machine calibration is essential for valid comparisons.
Future of Leads on ECG: Innovations and Trends
While the 12-lead ECG remains a staple, technological advancements are enhancing how leads on ecg are acquired and interpreted. From wearable devices to AI-powered analysis, the future is promising.
Wearable ECG Monitors and Mobile Apps
Devices like the Apple Watch, AliveCor KardiaMobile, and Zio Patch offer single-lead or multi-lead ECGs outside the clinic. While not a replacement for 12-lead ECGs, they enable early detection of arrhythmias like AFib.
- Provide continuous monitoring for high-risk patients.
- Enable patient-initiated recordings during symptoms.
- Limited spatial resolution compared to full 12-lead.
These tools complement traditional leads on ecg by increasing accessibility and early intervention.
Artificial Intelligence in ECG Interpretation
AI algorithms are being trained to interpret ECGs with high accuracy. They can detect subtle patterns missed by humans, such as early signs of hypertrophic cardiomyopathy or low ejection fraction.
- May reduce interpretation errors.
- Can prioritize critical ECGs in emergency queues.
- Still requires clinical validation and oversight.
For research on AI in ECG, see Nature Medicine – AI ECG Study.
Expanded Lead Systems and 3D Mapping
Some advanced systems use 80- or 120-lead body surface mapping to create 3D electroanatomical models of the heart. These are used in electrophysiology labs for ablation planning.
- Provide higher spatial resolution.
- Help localize arrhythmia foci with precision.
- Currently limited to specialized centers.
These systems represent the next evolution of leads on ecg, offering unprecedented detail.
What do the 12 leads on ECG represent?
The 12 leads on ECG represent different electrical viewpoints of the heart. Six limb leads (I, II, III, aVR, aVL, aVF) provide a frontal plane view, while six precordial leads (V1–V6) offer a horizontal plane view. Together, they allow comprehensive assessment of cardiac electrical activity.
How are leads on ECG used to diagnose a heart attack?
Leads on ECG detect myocardial infarction by showing ST-segment elevation or depression in specific leads. For example, ST elevation in leads II, III, and aVF indicates an inferior MI, while elevation in V1–V4 suggests an anterior MI. Reciprocal changes and Q waves also support the diagnosis.
What happens if ECG leads are placed incorrectly?
Incorrect lead placement can lead to misdiagnosis. For example, swapping arm electrodes can mimic dextrocardia or MI. Misplaced chest leads can alter QRS progression or create false ST changes. Proper training and anatomical landmarks are essential to avoid errors.
Can a 12-lead ECG be done at home?
While full 12-lead ECGs require professional equipment, some portable devices offer limited lead recordings. Wearables like KardiaMobile provide single-lead ECGs for rhythm monitoring, but they cannot replace the diagnostic power of a full 12-lead ECG performed in a clinical setting.
Why are leads on ECG important for heart health?
Leads on ECG are crucial because they provide spatial information about the heart’s electrical activity. This allows clinicians to localize damage, diagnose arrhythmias, detect hypertrophy, and guide life-saving treatments. Without accurate leads, critical conditions might be missed or misdiagnosed.
Understanding leads on ECG is fundamental to cardiac care. From the basic limb and chest leads to advanced interpretation and emerging technologies, these electrical viewpoints offer a window into the heart’s function. Whether diagnosing a heart attack, detecting arrhythmias, or monitoring treatment, the 12-lead ECG remains an indispensable tool. As technology evolves, the principles of lead placement and interpretation will continue to underpin accurate and effective cardiac diagnosis.
Further Reading: