Understanding the correct leads ecg placement is crucial for accurate heart monitoring—yet it’s one of the most commonly misunderstood procedures in clinical settings. Get it wrong, and you risk misdiagnosis, delayed treatment, or even life-threatening errors.
What Is Leads ECG Placement and Why It Matters

Electrocardiography (ECG or EKG) is a fundamental diagnostic tool used to assess the electrical activity of the heart. At the core of this process lies the correct placement of ECG leads—electrodes attached to the skin that detect and transmit cardiac signals to the ECG machine. Proper leads ecg placement ensures that the resulting waveform accurately reflects the heart’s rhythm, conduction, and overall function.
Incorrect lead positioning can distort the ECG reading, leading to false interpretations such as misdiagnosing myocardial infarction, arrhythmias, or electrolyte imbalances. According to the American Heart Association (AHA), up to 40% of resting ECGs may contain lead misplacement errors, significantly affecting patient outcomes. This makes mastering leads ecg placement not just a technical skill, but a critical component of patient safety.
The Science Behind ECG Lead Systems
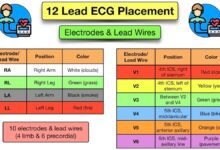
An ECG uses a standardized system of 12 leads to capture the heart’s electrical activity from multiple angles. These leads are derived from 10 electrodes placed on the limbs and chest. The system includes:
- 3 standard limb leads (I, II, III)
- 3 augmented limb leads (aVR, aVL, aVF)
- 6 precordial (chest) leads (V1–V6)
Each lead provides a unique vector view of the heart’s depolarization and repolarization. For instance, lead II is particularly sensitive to inferior wall activity, while V1 and V2 focus on the septal region. Misplacing even one electrode can shift these vectors, altering the morphology of the QRS complex, ST segment, or T wave.
“The ECG is only as good as the lead placement.” – Dr. Eric Topol, renowned cardiologist and digital medicine pioneer.
Historical Evolution of ECG Lead Placement
The foundation of modern ECG lead placement was laid by Willem Einthoven in the early 20th century. His invention of the string galvanometer and the development of the three limb leads (I, II, III) earned him the Nobel Prize in 1924. Over time, the system was expanded by Frank Wilson and colleagues, who introduced the concept of unipolar leads and the central terminal, leading to the development of the augmented limb leads (aVR, aVL, aVF).
In the 1940s, the precordial leads (V1–V6) were standardized by the American Heart Association, completing the 12-lead ECG system still in use today. Despite over a century of refinement, variations in training and practice continue to cause inconsistencies in leads ecg placement across healthcare facilities.
Step-by-Step Guide to Correct Leads ECG Placement
Performing a 12-lead ECG requires precision, consistency, and adherence to anatomical landmarks. Below is a detailed, step-by-step protocol to ensure accurate leads ecg placement.
Limb Lead Placement: Precision on Arms and Legs
The four limb electrodes form the basis of the hexaxial reference system used to calculate the heart’s electrical axis. Their correct placement is essential for accurate limb lead readings.
- Right Arm (RA): Place the electrode on the right forearm, just above the wrist. Avoid bony prominences or areas with muscle movement.
- Left Arm (LA): Position symmetrically on the left forearm, mirroring the RA placement.
- Right Leg (RL): Attach to the right lower leg, above the ankle. This serves as the electrical ground.
- Left Leg (LL): Place on the left lower leg, completing the circuit.
While these electrodes are often placed on the limbs, in cases of amputation or severe burns, they can be placed on the torso—proximal to the shoulders or hips—provided they are positioned symmetrically. However, this must be documented, as it can alter the ECG baseline.
Precordial (Chest) Lead Placement: Navigating the Thorax
The six chest leads (V1–V6) provide a horizontal plane view of the heart and are critical for diagnosing anterior, lateral, and septal myocardial infarctions. Their placement follows specific intercostal spaces and anatomical landmarks.
- V1: 4th intercostal space, immediately to the right of the sternum.
- V2: 4th intercostal space, immediately to the left of the sternum.
- V3: Midway between V2 and V4.
- V4: 5th intercostal space, along the midclavicular line.
- V5: Horizontal to V4, along the anterior axillary line.
- V6: Horizontal to V4 and V5, along the midaxillary line.
Accurate identification of the 4th and 5th intercostal spaces is crucial. To locate the 4th ICS, first find the sternal angle (Angle of Louis) at the 2nd rib level. Move down two spaces to reach the 4th ICS. Misplacement of V1 or V2 by even one intercostal space can mimic anterior ischemia or mask a true STEMI.
The National Heart, Lung, and Blood Institute (NHLBI) emphasizes that “precise electrode placement is non-negotiable for diagnostic accuracy.” Learn more about ECG standards at NHLBI.
Common Errors in Leads ECG Placement and Their Consequences
Despite its routine nature, ECG lead misplacement is alarmingly common. Studies show that up to 50% of ECGs in emergency departments contain at least one lead placement error. These mistakes can have serious clinical implications.
Reversed Limb Electrodes: A Frequent but Dangerous Mistake
One of the most common errors is the reversal of right and left arm electrodes. This causes significant changes in the ECG, including:
- Inversion of P waves, QRS complexes, and T waves in leads I and aVL
- Apparent right axis deviation
- Mimicry of dextrocardia or complex arrhythmias
While experienced clinicians may recognize these patterns, in high-pressure environments like the ER, such artifacts can lead to unnecessary interventions. A simple mnemonic—”White on Right”—can help prevent this: the white electrode goes on the right arm.
Incorrect Chest Lead Positioning: Hidden Risks
Misplacing chest leads is another frequent issue. For example:
- Placing V1 and V2 in the 3rd or 5th ICS can mimic anterior MI or obscure true ST elevation.
- Shifting V4–V6 too high or too lateral alters the R-wave progression, potentially leading to false diagnoses of left ventricular hypertrophy or posterior infarction.
- Failure to place V4 at the 5th ICS, midclavicular line, is particularly problematic in women with large breasts, where leads may be placed too high or too medially.
A 2020 study published in the Journal of Electrocardiology found that 32% of ECGs in a tertiary care hospital had at least one precordial lead misplaced, with V2 and V4 being the most commonly affected. Read the full study here.
Special Considerations in Leads ECG Placement
While standard protocols apply to most patients, certain populations and conditions require modifications to ensure accurate leads ecg placement.
ECG in Women: Addressing Anatomical Challenges
Female anatomy, particularly breast tissue, can complicate chest lead placement. The standard position for V3–V6 may be obscured by breast tissue, leading technicians to place electrodes on top of the breast rather than underneath.
The correct approach is to lift the breast and place the electrode on the chest wall at the correct anatomical landmark. This ensures that the electrical signal is captured from the myocardium, not attenuated by soft tissue. The American College of Cardiology recommends this technique to avoid signal distortion.
Obese and Pediatric Patients: Tailoring the Approach
In obese patients, thick adipose tissue can dampen electrical signals, increasing noise and reducing ECG amplitude. To compensate:
- Use high-quality, adhesive electrodes with good skin contact.
- Shave excess hair and clean the skin with alcohol to reduce impedance.
- Consider using alternative lead systems like the Mason-Likar modification for stress testing.
For pediatric patients, electrode size must be appropriate for body size. Neonates and infants may require smaller electrodes, and lead placement may need adjustment based on body proportions. The V4 placement, for instance, may be at the 4th ICS in very young children.
“In pediatrics, one size does not fit all—lead placement must be age and size appropriate.” – Pediatric Electrocardiography Guidelines, American Heart Association.
Advanced Techniques and Alternative Lead Systems
While the standard 12-lead ECG is the gold standard, alternative lead systems and advanced techniques can enhance diagnostic accuracy in specific scenarios.
Mason-Likar Modification: When Limb Leads Are Relocated
The Mason-Likar system is often used during stress testing or when limb movement interferes with signal quality. In this modification:
- Limb electrodes are moved to the torso: RA near the right clavicle, LA near the left clavicle, RL and LL near the hips.
- Precordial leads remain unchanged.
This reduces motion artifact but alters the limb lead voltages and axis. Therefore, ECGs using this system should be clearly labeled to avoid misinterpretation.
leads ecg placement – Leads ecg placement menjadi aspek penting yang dibahas di sini.
Right-Sided and Posterior ECGs: Expanding Diagnostic Scope
In suspected right ventricular or posterior myocardial infarction, standard 12-lead ECG may miss critical changes. Right-sided ECGs involve placing V4R (mirror of V4) on the right side of the chest, which is highly sensitive for right ventricular infarction.
Posterior leads (V7–V9) are placed on the back, along the scapular and paraspinal lines, to detect posterior ST elevation. These are especially useful when anterior leads show tall R waves and ST depression—signs of reciprocal changes.
For more on extended ECG lead systems, visit ECG Waves, a trusted educational resource.
Training, Technology, and Quality Control in Leads ECG Placement
Ensuring consistent, accurate leads ecg placement requires a combination of proper training, technological support, and institutional quality control.
The Role of Education and Certification
Despite its importance, ECG lead placement is often taught briefly in medical and nursing programs. A 2018 survey of nursing students found that only 35% could correctly identify all six precordial lead positions.
To address this, many hospitals now require ECG competency certification for staff involved in ECG acquisition. Programs like the Alliance for ECG Excellence (AEHRS) offer standardized training and certification to improve accuracy and consistency.
Technological Aids: From Skin Markers to AI
Recent advancements aim to reduce human error in leads ecg placement:
- Skin markers: Reusable templates or adhesive guides help technicians locate intercostal spaces and anatomical landmarks.
- Digital ECG systems: Some machines now include real-time feedback, alerting users to potential lead reversals or poor signal quality.
- Artificial Intelligence: Emerging AI tools can detect lead misplacement by analyzing waveform patterns and comparing them to expected norms.
While technology aids accuracy, it cannot replace foundational knowledge. The human element remains central to high-quality ECG performance.
Legal and Ethical Implications of Incorrect Leads ECG Placement
Misplaced ECG leads are not just a technical oversight—they can have serious legal and ethical consequences.
Malpractice Risks and Patient Safety
Incorrect leads ecg placement can lead to diagnostic errors, delayed treatment, or inappropriate interventions. For example, a reversed arm lead causing apparent ST elevation might lead to an unnecessary cardiac catheterization.
In malpractice cases, failure to follow standard ECG protocols can be seen as a breach of the standard of care. Documentation of proper technique, including any deviations from standard placement, is essential for legal protection.
Professional Accountability and Best Practices
Healthcare providers have an ethical duty to ensure diagnostic accuracy. This includes:
- Verifying lead placement before recording.
- Labeling any non-standard placements (e.g., limb leads on torso).
- Participating in regular competency assessments.
Organizations like the AHA and the European Society of Cardiology (ESC) publish guidelines to support best practices. Adherence to these standards demonstrates professional responsibility and commitment to patient safety. Explore ESC ECG guidelines.
What is the most common leads ecg placement error?
The most common error is the reversal of the right and left arm electrodes, which inverts waveforms in leads I and aVL and can mimic dextrocardia or serious arrhythmias. This is often preventable with proper training and the use of the “White on Right” mnemonic.
How do you ensure accurate precordial lead placement?
Accurate precordial lead placement requires identifying the 4th and 5th intercostal spaces using the sternal angle (Angle of Louis) as a landmark. Electrodes V1 and V2 go in the 4th ICS, V4 in the 5th ICS at the midclavicular line, and V3, V5, V6 are placed relative to these. Use anatomical guides or templates when needed.
Can ECG leads be placed on the torso instead of limbs?
Yes, in cases of amputation, burns, or limb injury, limb electrodes can be placed on the torso (proximal to shoulders or hips). However, this alters the ECG baseline and must be clearly documented to avoid misinterpretation.
Why is leads ecg placement important for diagnosing heart attacks?
Correct leads ecg placement is essential for detecting ST-segment elevation myocardial infarction (STEMI). Misplaced leads can mask ST elevation or create false positives, delaying life-saving interventions like thrombolysis or PCI.
Are there special ECG lead placements for women?
Yes, in women with large breasts, chest leads V3–V6 should be placed on the chest wall beneath the breast tissue, not on top of it. Lifting the breast to place the electrode correctly ensures accurate signal transmission from the heart.
Mastering leads ecg placement is far more than a technical checklist—it’s a cornerstone of accurate cardiac diagnosis and patient safety. From the precise positioning of limb and chest electrodes to understanding the consequences of common errors, every step impacts the reliability of the ECG. With proper training, adherence to standards, and the support of emerging technologies, healthcare providers can minimize errors and deliver higher-quality care. Whether you’re a novice technician or an experienced clinician, never underestimate the power of correct leads ecg placement in saving lives.
leads ecg placement – Leads ecg placement menjadi aspek penting yang dibahas di sini.
Further Reading: